Comentarios de Prevención y promoción de la salud
Dieta y Actividad Física
El objetivo de reducir el tabaco está muy claro: reducir su consumo tanto como sea posible en las personas individuales y en los grupos de población, y crear, idealmente, un mundo libre de humo. Respecto a la dieta y a la actividad física, el objetivo está menos claro y continúa existiendo un intenso debate acerca de lo que se debería recomendar en ambos casos; lo mismo se aplica a decidir qué acciones generarán el mayor beneficio, para quienes y en qué condiciones.
La OMS recomienda estas directrices para las personas que deseen mejorar su dieta (10):
· Conseguir el balance energético y un peso saludable
· Limitar la ingesta de energía procedente de grasas totales y cambiar el consumo de grasas de las grasas saturadas a las insaturadas, para llegar a eliminar los ácidos grasos trans
· Aumentar el consumo de frutas y verduras, legumbres, granos enteros y frutos secos
· Limitar la ingesta de azúcares libres
· Limitar el consumo de sal de todos los orígenes y asegurarse de que la sal es yodada.
En relación con la actividad física, la OMS recomienda “como mínimo treinta minutos de actividad física regular y de intensidad moderada la mayoría de los días” (10).
Se espera que este nivel de actividad reduzca el riesgo de enfermedad cardiovascular, diabetes, cáncer de colon y cáncer de mama. Para controlar el peso es posible que se necesite más actividad. Una revisión Cochrane reciente de 43 ensayos aleatorios con 3.476 participantes descubrió que el ejercicio aumentaba la pérdida de peso en comparación con no hacer ningún tratamiento, pero que hacer régimen era más efectivo (11).
Las personas que hacían ejercicio perdieron de 0,5 a 4,0 kg, mientras que los sujetos seleccionados al azar en grupos sin tratamiento ganaron 0,7 kg o perdieron 0,1 kg. El ejercicio tenía más efecto en los factores de riesgo para la enfermedad cardiaca que en el peso, y el ejercicio más intenso provocaba una pérdida de peso mayor. Los efectos del ejercicio parecían ser diferentes en hombres y en mujeres, ya que las mujeres tenían que reducir su ingesta de calorías de forma más activa para perder peso. (12) Muchas personas con enfermedades crónicas múltiples no podrán realizar treinta minutos de ejercicio la mayoría de días, aunque, en contra de la opinión general, el Programa de Prevención de la Diabetes demostró que era más probable que las personas con sesenta años o más siguieran el consejo de hacer más ejercicio y de mejorar su dieta que los más jóvenes (13).
Aumentar la actividad física puede ser más beneficioso que mejorar la dieta en el sentido de que, además de reducir las posibilidades de desarrollar una enfermedad crónica, también mejora la calidad de vida, factor que puede ser especialmente importante para las personas que padecen una enfermedad crónica compleja (14).
Recientemente la OMS realizó un estudio sistemático de datos que demuestran lo que funciona al aumentar la actividad física y mejorar la dieta (15). Se analizaron los datos a partir de las siguientes categorías: política y medio ambiente, medios de comunicación, contextos escolares, lugar de trabajo, comunidad, atención sanitaria primaria, adultos mayores y contextos religiosos (Tabla 1).
Tabla 1. Estudio sistemático de las intervenciones orientadas a mejorar la dieta y promover la actividad física (15)
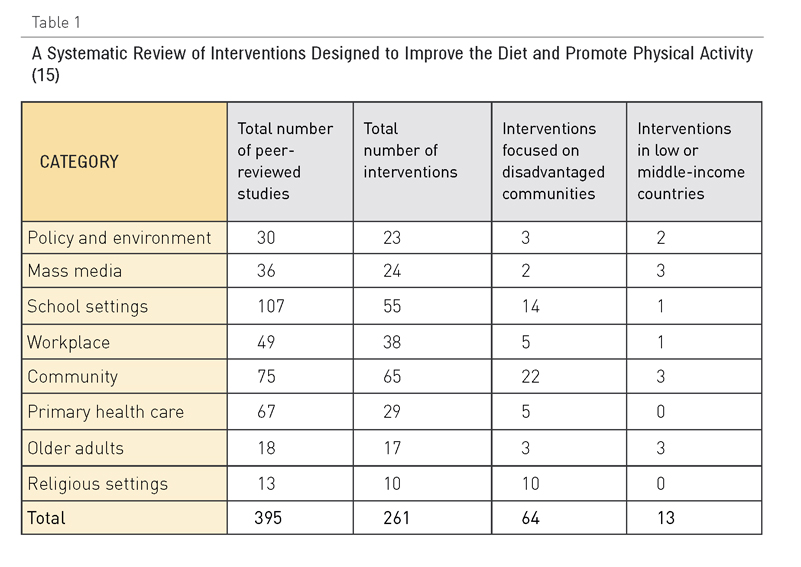
Los revisores identificaron 395 estudios que cumplían sus criterios de inclusión, pero solo trece de ellos estaban relacionados con países de rentas medias o bajas, y solo dieciocho se ocupaban de adultos mayores. El estudio tuvo en cuenta resultados psicosociales, actitudinales y clínicos y clasificó las intervenciones como eficaces, moderadamente eficaces, prometedoras pero basadas en pocas pruebas, mínimamente eficaces, basadas en pruebas insuficientes o con eficacia no demostrada, o con resultados que no se medían o recogían en el informe. Teniendo en cuenta las limitaciones de los estudios que se incluían en el análisis, las conclusiones principales del estudio se resumen en los puntos siguientes:
- Política y medio ambiente: Se encontraron tres intervenciones que resultaban eficaces: 1) regulación gubernamental que apoye alimentos básicos más sanos; por ejemplo, sustituir el aceite de palma por aceite de soja, con lo que se reduce el contenido en ácidos grasos en la dieta; 2) políticas de construcción, planificación y transporte que disminuyan las barreras para realizar actividad física, y 3) carteles en lugares estratégicos para fomentar el uso de las escaleras. Entre las intervenciones de eficacia moderada se encuentran las políticas de fijación de precios, los carteles en los puntos de venta para animar a elegir los productos más sanos y los enfoques dirigidos a un público amplio para animar a caminar más y a ir en bicicleta.
- Medios de comunicación: Las campañas para promover la actividad física son eficaces si se combinan con programas de apoyo basados en la comunidad o relacionados con políticas para reducir las barreras medioambientales que impiden la actividad física. Entre las intervenciones de eficacia moderada se encuentran las campañas intensivas que se concentran en un solo mensaje (como aumentar el consumo de leche semidesnatada), las marcas o logotipos de salud nacionales que indican a los consumidores cuáles son los alimentos más sanos y campañas intensivas a largo plazo que promueven dietas sanas.
- Contextos escolares: Los programas escolares de alta intensidad pueden funcionar si son globales y tienen muchos componentes, entre los que se incluyen la enseñanza impartida por personas con la formación necesaria, políticas escolares de apoyo, un programa de actividad física, un componente parental/familiar y la opción de elegir comida sana en las escuelas. Los programas y evaluaciones centrados en las necesidades de las escuelas y su contexto cultural tienen una eficacia moderada.
- Lugar de trabajo: Los programas multicomponenciales para el lugar de trabajo que incluyen el ofrecimiento de comida sana y espacios para realizar ejercicio, en los que se implica al personal para su planificación e implementación, se incorporan intervenciones familiares, se ayuda a las personas a cambiar, y se cuenta con supervisión, resultan efectivos.
- Comunidad: Hay tres intervenciones que han demostrado ser eficaces en la comunidad. En primer lugar, programas de educación para la dieta con muchos componentes orientados a grupos de alto riesgo. En segundo lugar, programas de desarrollo de la comunidad que suponen la cooperación intersectorial, o tienen un único objetivo, como reducir el riesgo de un acontecimiento cardiovascular. En tercer lugar, programas basados en la comunidad para un grupo homogéneo. Varias intervenciones han demostrado tener una eficacia moderada: utilizar los servicios de consultas telefónicas para pedir consejos sobre alimentación, intervenciones comunitarias realizadas como parte de una campaña nacional o global, programas que se dirigen a la población pobre o analfabeta y que incluyen consejos sobre alimentación, intervenciones basadas en la informática que ofrecen un feedback personalizado para grupos de alto riesgo, “tours” por el supermercado para apoyar la compra de alimentos más sanos, y el autobús escolar peatonal.
- Atención primaria: Las intervenciones de atención primaria que se dirigen a personas con riesgo de padecer una enfermedad crónica pueden ser eficaces si incluyen a personas que son inactivas, que comen menos de cinco porciones de fruta o verdura cada día, que consumen muchas grasas, que tienen sobrepeso o que cuentan con una historia familiar de enfermedad crónica; si incluyen como mínimo una sesión con un profesional de la salud que negocie objetivos razonables con un seguimiento por parte de personal cualificado, y si cuentan con el apoyo de información orientada al público objetivo. Las intervenciones vinculadas con acciones que llevan a cabo otros sectores interesados, por ejemplo, instituciones deportivas o medios de comunicación, también pueden resultar eficaces. Los programas que identifican a los pacientes con altos niveles de colesterol en la sangre y ofrecen seguimiento tienen una eficacia moderada, como también la tienen los programas para perder peso que incluyen consultas telefónicas o por internet a lo largo de un periodo de cuatro semanas como mínimo y un programa de autoayuda con autocontrol.
- Adultos mayores: A pesar de que el análisis sistemático encontró dieciocho estudios de diecisiete intervenciones en adultos mayores, no identificó ninguna intervención eficaz en este grupo de edad en concreto, lo que es muy destacable para nuestro interés por las personas con múltiples enfermedades crónicas. Entre las intervenciones de eficacia moderada se encontraban las que promueven la actividad física en un contexto de grupo que utilizaban una estructura social existente o un lugar de encuentro, y las intervenciones en el hogar en las que se ofrece a los adultos mayores un acceso más fácil a frutas y verduras utilizando una infraestructura existente.
- Contextos religiosos: Las intervenciones relacionadas con la alimentación, que cuentan con muchos componentes y son adecuadas culturalmente, que se planifican y se implementan junto con líderes religiosos e incluyen sesiones de educación en grupo y estrategias de autoayuda, resultan eficaces. Las intervenciones culturalmente adecuadas orientadas a perder peso, llevar una dieta sana y aumentar la actividad física tienen una eficacia moderada.
Este estudio identifica muchas intervenciones en las que hay pruebas que demuestran que son eficaces y luego se fija en las características que al parecer comparten las intervenciones que funcionan. Estas características suelen ser: un diseño multicomponencial, adaptación al contexto local tanto cultural como medioambientalmente, uso apropiado, estructuras sociales existentes y la necesidad de la participación de los sectores interesados a lo largo del proceso.
Los autores del estudio también indican que la mayoría de estudios son a corto plazo, lo que significa que la mayoría de los resultados son más psicosociales que clínicos, y que tenernos pocos datos acerca de la sostenibilidad del programa. Pocos de esos estudios ofrecían información acerca de la rentabilidad o tenían en cuenta las consecuencias no intencionadas.
Los pocos datos de los países con rentas bajas y medias indican claramente que es importante implicar a las comunidades en todas las fases de la planificación, implementación y evaluación para lograr el éxito.
En cuanto a las polipatologías, es realmente necesario que se lleve a cabo un estudio que tenga en cuenta estos procesos y enfoques y analice su relevancia respecto a la prevención, así como la trayectoria que lleva a la polipatología. Si se contara con X prácticas o políticas, ¿se podría reducir la incidencia de las enfermedades crónicas complejas y retrasar su inicio e impacto? ¿Qué grupos de población tienen mayor riesgo de padecer una enfermedad crónica compleja? ¿Deberíamos centrarnos en grupos de población de alto riesgo en términos de política y de intervención sanitaria para la población? ¿Qué esfuerzos son necesarios para que se produzcan cambios en estos grupos de población? ¿Qué análisis se necesitan?
Un análisis exhaustivo de los barrios y la diabetes en Toronto, Canadá (ICES, 2007), ofrece información muy valiosa acerca del contexto social y físico como factor determinante de la enfermedad crónica y de quiénes tienen más riesgo, y acerca de los enfoques que pueden resultar útiles para reducir su incidencia. Esta investigación es un buen ejemplo de los nuevos enfoques del estudio de la polipatología y su prevención (16).
Comentarios existentes
El horario laboral continuado al que nos quieren dirigir acabará totalmente con los beneficios de la dieta mediterranea. ¿Que hay de malo en poder ir a casa a comer comida casera y pasar un rato con la familia?
Me gustaría ser realista, dejar de lado los tecnicismos y contar lo que veo día a día, en la infancia y adolescencia se les inculca alimentación saludable en los colegios tanto por parte del profesorado como incluso nosotros mismos en charlas periódicas, pero resulta que los niños y adolescentes no comen, por lo general, frutas ni verduras y además existe una importante prevalencia de obesidad en estas franjas etarias; en edades medias de la vida nos hartamos de indicar a las personas el como deben alimentarse en pro de un mejor estado de salud y nos encontramos con que en la mayoría de las ocasiones al salir de la consulta suelen hacer lo que les viene en gana o lo que culturalmente vienen haciendo cotidianamente por decirlo de una manera mas suave.Entre todos ellos me encuentro alguno, los menos, caminando de cuando en cuando. La tercera parte del cupo de enfermos ya tiene mas de 65 años y muchos de ellos poliartrósicos que no pueden mas que caminar para ir a casa de la vecina de frente y ya es mucho pedir, y con unos hábitos dietéticos imposible de cambiar.
Todo lo expuesto no quiero que se interprete como una visión pesimista del problema sino que seamos conscientes del mucho trabajo a realizar en este campo y la dificultad que entraña conseguir metas sin que nos lleve al desánimo.
Las conclusiones de los estudios sobre dieta y ejercicio físico deberían hacerse más públicas de fácil acceso a toda la población, para que así también ellos pudieran aportar y exigir esas medidas.
Me gustaría comentar que en la edad adulta, ha un porcentaje de personas, que si bien tambien hay que modificar hábitos, no comen con tanto exceso, en cambio hay una falta de actividad física, que sería el denominador de la obesidad y de determinadas enfermedades. A veces insistimos mucho en la alimentación y poco en la actividad física
Otro comentario la palabra "dieta", es muy restrictiva e implica limitación en la comida, creo que es mejor que se hable de alimentación saludable o algo similar
Las recomendaciones de actividad física segón la OMS para personas mayores de 65 años en adelante consisten en actividades recreativas o de ocio,
desplazamientos (por ejemplo, paseos caminando o en bicicleta), actividades ocupacionales (cuando la persona
todavía desempeña actividad laboral), tareas domésticas, juegos, deportes o ejercicios programados en el contexto
de las actividades diarias, familiares y comunitarias.
Con el fin de mejorar las funciones cardiorrespiratorias y musculares y la salud ósea y funcional, y de reducir el riesgo
de ENT, depresión y deterioro cognitivo, se recomienda que:
1. Los adultos de 65 en adelante dediquen 150 minutos semanales a realizar actividades físicas moderadas
aeróbicas, o bien algún tipo de actividad física vigorosa aeróbica durante 75 minutos, o una combinación
equivalente de actividades moderadas y vigorosas.
2. La actividad se practicará en sesiones de 10 minutos, como mínimo.
3. A fin de obtener mayores beneficios para la salud, los adultos de este grupo de edades deberían aumentar
hasta 300 minutos semanales la práctica de actividad física moderada aeróbica, o bien acumular 150 minutos
semanales de actividad física aeróbica vigorosa, o una combinación equivalente de actividad moderada y
vigorosa.
4. Los adultos de este grupo de edades con movilidad reducida deberían realizar actividades físicas para mejorar
su equilibrio e impedir las caídas, tres días o más a la semana.
5. Convendría realizar actividades que fortalezcan los principales grupos de músculos dos o más días a la semana.
6. Cuando los adultos de mayor edad no puedan realizar la actividad física recomendada debido a su estado de
salud, se mantendrán físicamente activos en la medida en que se lo permita su estado.
En conjunto, considerando los tres grupos de edades, los beneficios que pueden reportar las actividades aquí
recomendadas y la actividad física en general son mayores que los posibles perjuicios. Cuando se invierten 150
minutos semanales en actividades de intensidad moderada, las tasas de lesión del aparato locomotor son muy bajas.
Para la población en general, el riesgo de lesiones del aparato locomotor podría disminuir si se fomentase un plan de
actividad física inicialmente moderado, que progresara gradualmente hasta alcanzar una mayor intensidad.
La actividad fisica y la dieta esta demostrado que influyen en la prevalencia de enfermedades cronicas, es fundamental una buena educacion en este sentido y segun este estudio de la OMS la intervencion es menos eficaz en adultos mayores , con malos habitos ya adquiridos, por lo cual tenemos que poner mas empeño en este tramo de poblacion, fomentando la actividad fisica incluso mas que la dieta.
Las medidas sobre la dieta y ejercicio físico esta bien que comience en las edades tempranas de la vida para así fortalecer habitos saludables pero no debemos olvidarnos de las edades medias y avanzadas de la vida ya que la mayoría de las actuaciones son llevadas a cabo en la prevencion secundaria, al ser las campañas gubernamentales muy escasas para el resto develas edades que no son la infancia y la adolescencia.
Se debe cambiar muchos habitos de vida que se han impuesto en las ultimas décadas en nuestra sociedad
La educación en dieta y ejercicio debería de imponerse para todos los públicos y todas las edades. Cada vez nos movemos menos y comemos mas, desde los pequeños a los mayores. Pienso que el sedentarismo y la dieta no saludable nos ha llevado a la situación actual donde las enfermedades cardiovasculares encabezan el ranking cuando hablamos de mortalidad.
Desde los colegias, a la publicidad, a la empresas, a los gobiernos etc, todo debería de favorecer y fomentar el ejercicio y la dieta sana. Pienso que es el origen de muchos de nuestros problemas y por tanto el mayor foco de intervención.
Creo que uno de los objetivos fundamentales en la prevención primordial es la educación infantil y juvenil, pero no solo a nivel de las escuelas, sino a nivel de la familia. Aquí incluiría políticas de conciliación familiar que permitan a los padres preocuparse de la alimentación de sus hijos y de realizar actividad física conjunta para crear el hábito.
Me sumo a la pregunta de por qué las personas no asumen la responsabilidad de conductas poco saludables y cuando llega el momento prefieren mantenerlas y que otros le solucionen el problema de forma fácil (si pueden, claro).
Una pregunta por comentario:
¿porque es tan difícil modificar un hábito de comportamiento insano y tan fácil tomarse una pastilla?
¿porque la población espera del sector salud un remedio que les permita una conducta insana?
¿porque la responsabilidad de nuestras acciones, pensamos que no tienen trascendencia cuando se habla de salud?
las claves del éxito de estas intervenciones preventivas recaen en la variedad, en el intervenir desde varios niveles y lugares, actuar desde las edades tempranas....
Poner a las personas como los protagonistas activos de su propio estado de salud, con la formaicón y el apoyo necesario, pero intervenir desde varios niveles y desde diversas iniciativas. Hacer más para dejar de adoptar posturas "más cómodas" y pasivas como puede ser la toma de una pastilla