Comentarios de Prevención y promoción de la salud
Consumo de tabaco
El consumo de tabaco mata a cinco millones de personas cada año en total, y puede que esa cifra aumente hasta diez millones para 2030 (4). La mitad de los fumadores muere prematuramente a consecuencia del tabaco y, sin embargo, si las personas dejan de fumar, pueden volver a tener el mismo riesgo que los no fumadores una vez transcurridos de diez a quince años.
En todo el mundo se ha reconocido el gran peligro que representa el tabaco y, en consecuencia, la OMS, por ejemplo, ha creado la Convención Marco para el Control del Tabaco, que obliga a los países a regular las ventas de tabaco, reducir la demanda de tabaco por parte de los consumidores, mejorar el medio ambiente y la salud de los trabajadores del sector tabaquero y fomentar la investigación. Un total de 168 países de los 192 posibles han firmado la Convención; Estados Unidos e Indonesia son los países más grandes que no han seguido el ejemplo.
Sabemos mucho acerca de las medidas de salud pública que resultan eficaces para reducir el consumo de tabaco. La OMS ha recopilado el paquete MPOWER (acrónimo que corresponde a las iniciales de las políticas en inglés), que recoge seis políticas que se sabe que funcionan (4).
Se trata de lo siguiente:
- Supervisar el consumo de tabaco y las políticas de prevención
- Proteger a las personas del humo del tabaco
- Ofrecer ayuda para dejar de consumir tabaco
- Avisar acerca de los peligros del tabaco
- Hacer respetar las prohibiciones referentes a la publicidad, la promoción y el patrocinio del tabaco
- Subir los impuestos del tabaco.
Es necesario apoyar la investigación en una serie de ámbitos: el control del tabaco, encuestas de los niveles de consumo de tabaco, el consumo global de cigarrillos, los efectos económicos en cada país (el tabaco conlleva pérdidas, no ganancias, ya que los costes de los daños causados sobrepasan los ingresos obtenidos a través de los impuestos), el coste del tabaco para los empresarios, los costes económicos de los incendios y de la basura generada, los costes para los fumadores, los documentos de las empresas tabaqueras, los litigios, la industria tabaquera y la contratación de científicos para la causa de las compañías tabaqueras.
Prohibir fumar en los lugares de trabajo y en los lugares públicos y aumentar los impuestos que gravan el tabaco son dos de las intervenciones más eficaces (4).
Figura 1—Eficacia de diferentes formas de terapia sustitutiva con nicotina a la hora de ayudar a las personas a dejar de fumar
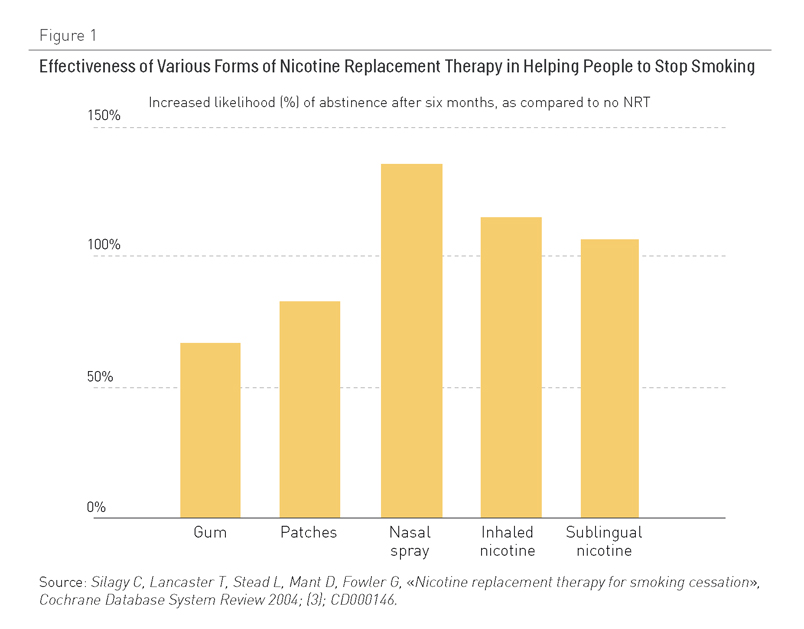
La figura 1 muestra datos extraídos de la revisión Cochrane sobre las tasas de personas que dejan de fumar tras probar varias formas de terapia sustitutiva con nicotina (4,5). La gran mayoría (entre dos tercios y tres cuartos) de ex-fumadores dejan de fumar completamente sin ayuda (6,7). Este dato proviene de países que cuentan con una experiencia de veinte años fomentando de forma importante las terapias sustitutivas con nicotina, que utilizan presupuestos que hacen parecer pequeño el gasto de las campañas públicas para dejar de fumar.
La mayoría de fumadores (de largo) dejan el tabaco tras estar expuestos a políticas y campañas de alcance general y al cambio cultural respecto al tabaco. No utilizan medicamentos, ni asisten a terapia ni recurren a líneas telefónicas para ayudar a dejar de fumar. Este es un mensaje importante y muy positivo.
Casi todos los ensayos de terapia sustitutiva con nicotina se han realizado en países ricos. Estos países se diferencian considerablemente de los países de renta baja y media en lo que se refiere a su cultura de control del tabaco (fumar está mucho mejor visto en la mayoría de países de rentas bajas y medias; en la mayoría de ellos, el control sobre el tabaco es escaso, y se realizan pocas campañas para motivar a la gente a dejar de fumar). No es aconsejable esperar un interés similar en las terapias sustitutivas con nicotina por parte de la población en los países en los que la mayoría de fumadores de hoy en día están vivos.
Los países que han impuesto prohibiciones generales a la publicidad (entendiéndose prohibiciones en la publicidad en los medios y en los puntos de venta) han sido testigos de una disminución mucho mayor del consumo de tabaco que los países que no han introducido este tipo de prohibiciones (4,8). Claramente hay varios aspectos a tener en cuenta en cuanto a la causalidad en este caso, pero las pruebas que demuestran la eficacia de las prohibiciones generales son significativas. Reducir los impuestos sobre el tabaco hace aumentar el consumo, y subir los impuestos, lo reduce (4,9). Esta sensibilidad hacia el precio se ha comprobado de forma repetida en muchos países en diferentes momentos, y está bien consolidada.
Muchos de los datos acerca de reducir el daño que provoca el tabaco se centran en los cigarrillos, pero en muchas regiones del mundo, como por ejemplo el sur de Asia, son habituales otras formas de tabaco fumado, como los bidis y el tabaco oral que no produce humo, especialmente entre las mujeres y los jóvenes.
Algo de lo que sabemos mucho menos es el efecto de estas políticas, incluida la terapia sustitutiva con nicotina, en pacientes con enfermedades crónicas complejas. De hecho, de unas cuarenta revisiones Cochrane acerca de dejar de fumar, ninguna se refería a pacientes que tuvieran una enfermedad crónica establecida. Es habitual que todo un conjunto de ensayos excluyan las polipatologías o mantengan un control sobre ellas.
También es importante reconocer que el control del consumo de tabaco resulta mucho más difícil por la presencia de una poderosa industria tabaquera cuyo objetivo es promover las ventas de tabaco en todo el mundo. Estas empresas cada vez concentran más sus energías en los países de rentas bajas y medias, donde el número de fumadores y de fumadores potenciales es significativo y los controles pueden no ser muy estrictos. Estos países dependen a menudo del tabaco para su desarrollo económico.
Comentarios existentes
Las politicas antitabaco siempre deben ser agresivas, aunque supongan un precio politico a priori.
Con respecto al comentario 7, creo que lo hacemos. Y también es importante que se haga en los colegios, centros culturales y fundamentales las campañas publicitarias realizadas por personajes de referencia para los jovenes y adolescentes.
Estoy de acuerdo con el compañero que menciona, la intervención breve antitabaco en la consulta de Atención Primaria como una de las medidas más coste-efectivas para conseguir el abandono del hábito tabáquico en la población general, no obstante, me pregunto ¿porqué no generalizamos esta actitud en nuestras consultas todos los profesionales sanitarios y no sanitarios que trabajamos para estos pacientes? ¿olvidamos una de las prácticas que ha demostrado mayor eficacia para promover la salud?.
Ah, y sobretodo, demos ejemplo y hagamos que nuestros pacientes no vea que nosotros hacemos luego lo que le decimos a ellos que no hagan.Un saludo.
Creo que el riesgo de consumo de tabaco es conocido por una gran parte de la poblacion. Una vez hecha la difusión , se esta implantando una politica restrictiva. Esto ha conseguido que un grupo de poblacion lo deje o al menos se lo plantee.
Aun así tenemos una parte importante que no se lo plantea con lo cual se tendrá que seguir insistiendo en las medidas implantadas.
Creo que toda politica encaminada al disminuir el consumo de tabaco es adecuada. En el ambito sanitario la actuacion mas eficaz sería el consejo antitabaco y el fomentar los programas y la informacion, sobre todo entre los jovenes.
Realmente las medidas descritas en este apartado, sobre los condicionantes externos para abandonar el hábito tabáquico, son realmente importantes, pero desde mi punto de vista lo más eficaz es retrasar la edad de incicio, interviniendo en el colegio y en el instituto, con programas informativos y de prevencion como la consulta joven.
Creo que las politicas antitabaco son esenciales. Ya sea con subida de impuestos, informando a los ciudadanos de sus consecuencias, como prohibiendo que se fume en lugares cerrados, ya sean públicos o privados. Con independencia de los resultados de las encuestas iniciales en relación con el consumo, creo que es necesario esperar más tiempo para evaluar el impacto en salud.
Me queda duda si se han estudiado las recaídas en el hábito, y en relación a qué método para dejar de fumar, incluidas las medidas políticas, es el más efectivo para evitar dichas recaídas.
En cuanto a datos sobre el abandono del tabaco en el paciente con enfermedades crónicas, supongo que la seriedad con que se lo tome dependerá del tipo de patología y de la relación que él mismo encuentre entre su enfermedad y el tabaco. Por ejemplo un enfermo coronario o pulmonar, relaciona tabaco a su enfermedad con mayor facilidad que un enfermo renal p.e. Yo observo que un enfermo renal con patología pulmonar asociada, abandona el tabaco con más facilidad que aquél que no presenta la pulmonar por mucho que se le explique la importancia. Quizá falte ese tipo de difusión de información en las campañas.
Desde la ley antitabaco en España, según dicen, las últimas encuestas, sólo un 6% de quienes se palntearon dejar de fumar lo han hecho.
Evidentemente, las personas fumadoras pasivas agradecen la ley, son las más beneficiadas.
Sin embargo, pienso que las encuestas llevan intereses, a pesar del no abandono total, si en 7 horas de trabajo no puedo fumar, en el día voy a fumar menos. El consumo de tabaco habrá descendido, por lo tanto los datos en la evidencia que aporta el documento pongo en cuestión la encuesta recientemente publicada.
Estoy de acuerdo que las políticas antitabaco tienen que ser contundentes y con una educación sanitaria desde la infancia y a lo largo de la vida